Which Corona strategy does the Netherlands actually have? Time for a thorough analysis of what we are doing and where we are headed.
By Mick Blok - June 25th, 2020
Summary
The Netherlands does not have a clear Corona policy. That is bad enough as it is. What is worse: there is little evidence that the Netherlands has any desire to get rid of the virus. Our analysis shows that all actors behave and express themselves in a contradictory fashion. Although the Outbreak Management Team recently defined the policy of "maximum control" as "suppressing" the spread "as much as possible" to "(almost) zero", the RIVM institute defines the same concept as merely slowing the epidemic down. And the same OMT is now OK with a rising number of infections. That's not suppression.
Our best guess is that, at the moment, RIVM and GGD-GHOR are still aiming for a controlled spread of the virus and the gradual build-up of immunity, and the OMT is going along with this for now, despite the fact that since 23 June it has paid lip service to the concept of "suppression", and the media and the cabinet do not grasp the difference between "some virus circulation" and "no virus circulation".
In a situation where one has a diffuse, multiplicitous strategy, however, the strategy that suppresses the virus least "wins". Therefore, our major discrepancies in the Corona strategy are in dire need of clarification.
Preface
From the kick-off of the Dutch Corona strategy on 16 March to the present day, there has been confusion about the policy. This confusion is not good for public support for mitigation measures and makes rational debate about where we want to go impossible.
“We cannot rule out the possibility that the Netherlands lack a strategy and only react to societal pressure."
And with that, confusion about policy is perhaps as bad as the wrong policy. We also have to take into account that the Netherlands has no strategy and only responds to societal forces. Because the people have so much confidence in the authorities and the media participate in the "we're all good here" frame, there is no pressure to choose a strategy.
We analyze where the Netherlands is now, with as neutral as possible a "bird's eye view".
When Prime Minister Rutte announced in March that the Netherlands would allow the Corona virus to spread through the population as long as the hospitals did not get too full, the strategy was fairly clear. Spreading the virus infects people, they become immune, which puts a brake on the virus for the others. But the spread should not be allowed to go too quickly, because then hospitals would overflow. This may not have been an attractive policy, nor has it won any beauty awards in the performance, but at least it was clear.
Policy has since shifted. When Rutte makes sounds like “as little as possible” in recent weeks, this is fundamentally different from March. But the RIVM site and other policymakers are still talking about the old policy. And there has been no clear statement such as “we are going to zero and we will stay there as long as possible”.
Which strategic options exist?
Because debate and policy now depend on subtleties, it is necessary to describe subtle differences in policy (bear in mind: differences that are not subtle in terms of outcomes such as mortality and economic damage). We distinguish four strategies and their internal logic:
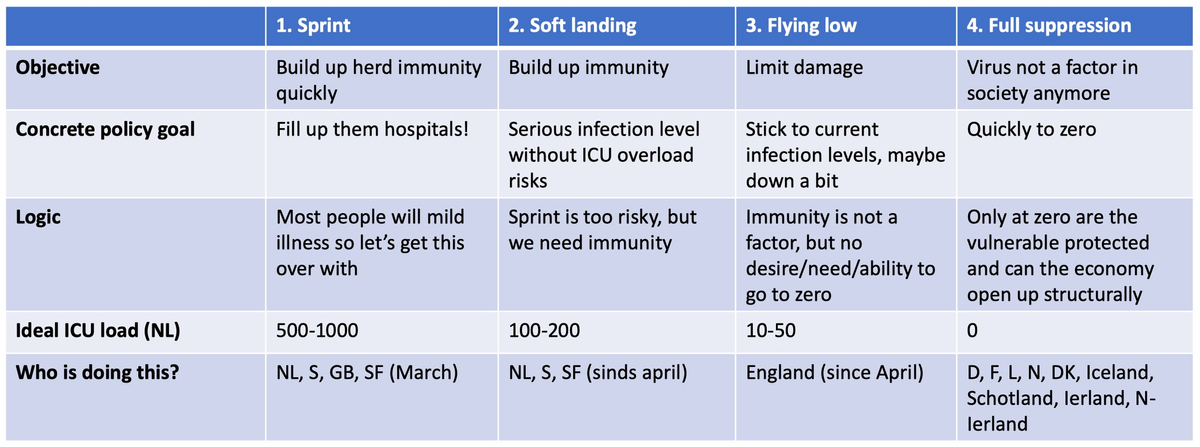
1. The Sprint.
This seems to have been the aim of RIVM (Dutch CDC) director Jaap van Dissel in March. The data from China indicated that the outbreak had gone very quickly, with relatively few deaths, and had been extinguished because enough people had built up immunity. By allowing serious infections for 1 or 2 months, you can then control the outbreak with limited measures (washing hands, no discos) or no measures (if you have achieved full 60% herd immunity). The economy can then be opened up (almost) completely.
2. The soft landing.
By building up immunity steadily but not very quickly, you will achieve similar goals as with the Sprint, but without the great risk that the hospitals will fill up. By accepting infections you can, at least in the short term, open the economy relatively faster. At least, that is the theory.
3. Flying low.
You open the economy as quickly as you can without accepting an increase in infections. It always drops a little or remains very low, but little value is attached to going to zero. This makes sense if you estimate the health damage from the virus to be limited. This can also seem like an attractive strategy if you don't think you can get to full repression at all, for example because you don't believe in the power of mass testing, tracing and isolation and/or masks.
4. Full suppression.
You try to go to zero infections and then occasionally knock down an outbreak, if necessary. This is attractive if you think that suppression is possible (with a lot of testing, good contact research and possibly other measures such as masks in public areas), if you think that the virus is very dangerous or if you see that the world is suppressing and you are becoming an outcast. This is also the strategy you choose if you are concerned that there will never be a vaccine or that a vaccine would not be used enough to get herd immunity. Because if you allow a little or quite a lot of infections to exist, you are simply "wearing down" your population until just about everyone has lung complaints.
For us, the struggle has been (since March) to get Strategy 4 accepted and implemented. This virus is too dangerous to allow its circulation, if you let it circulate you have a much higher risk of a major new outbreak, and other countries are showing that suppression can actually be relatively painless with lots of testing, good contact research and masks in public areas.
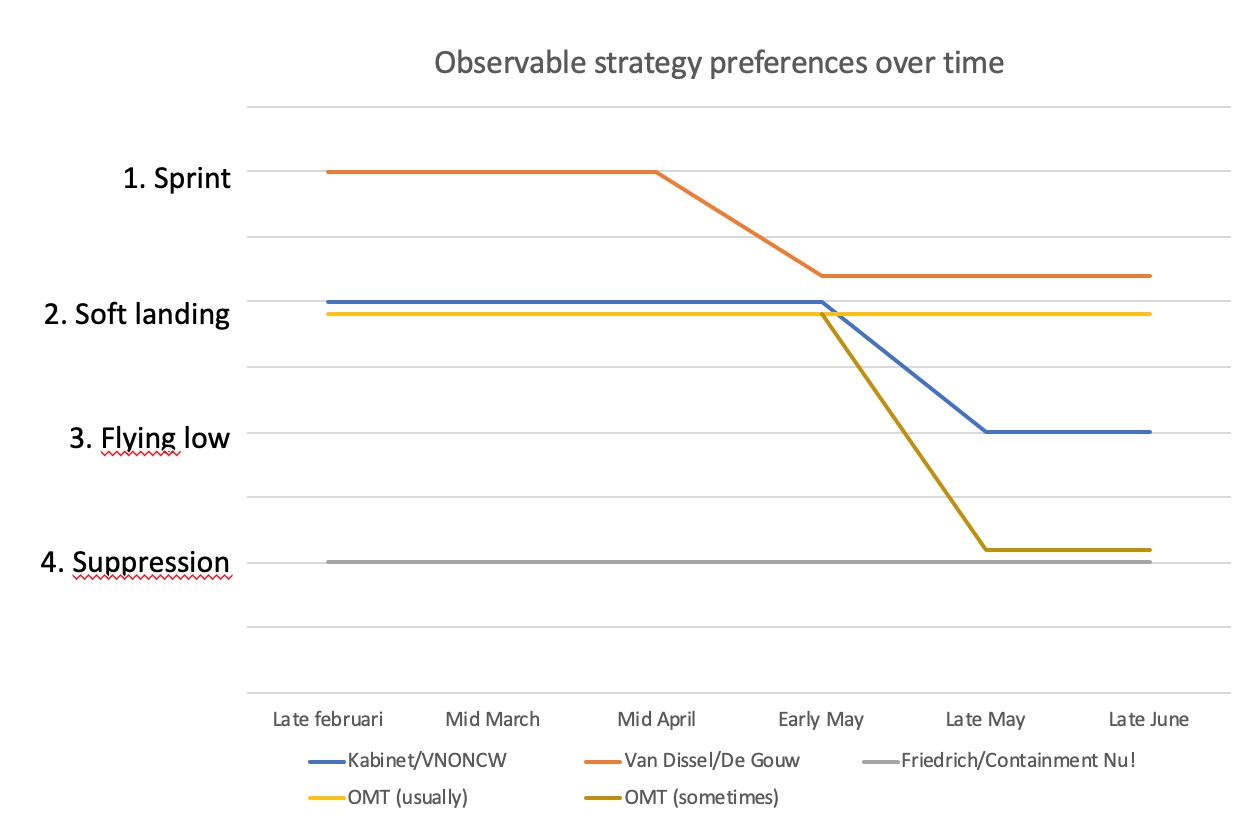
In the graph below, we analyze indicatively where we think the actors stand on this issue, over time from February to now.
How can we analyze what the government really intends to do? What will happen with the outbreak and the country? Can we trust that the outbreak can be kept under control? There are 8 ways to analyze that (we promised to be thorough):
- The official policy, as announced and posted on the government's websites
- The statements of policymakers
- The signal values in the government Corona Dashboard
- The real-life actions of the government
- The communication and information provision from the government
- The results of the policy
- The internal logic and interests
- Reverse logic: what would we observe if the policy were different?
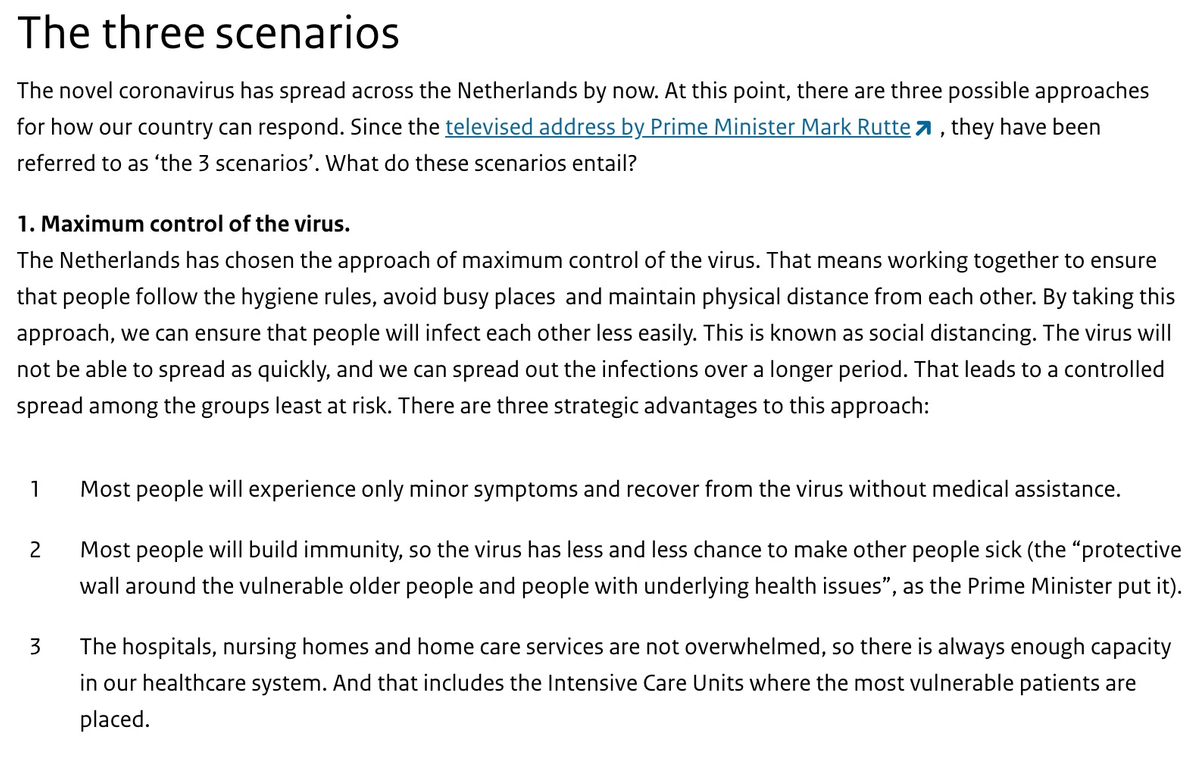
1. Official policy
The policy was announced in the first Dutch National Address in nearly half a century on March 16, and has never been officially modified since. If a National Speech is to have value and credibility, then that policy will be in place until it is clearly and officially changed again. A simple principle. Rutte will have to look into the camera and use words such as “towards zero”, “national effort to suppress the virus” and “it was a mistake to have immunity-building as an objective”. Until he does, his policy is to spread the virus, by default. Those who hope that this is not the case apparently feel it is more painful to believe that the policy is weird than that our national leader just plays around a bit with a National Address.
But there is more that makes us believe that the policy has not changed. To the present day, the RIVM site has the same policy as since mid-March: ensuring that hospitals are not overburdened and protecting vulnerable groups (which means building up immunity for the non-vulnerable). Such targets could be compatible with Strategy 2, but point to Strategy 1 because you don't want to keep “vulnerable” groups indoors for 5 years before the build-up of immunity protects them. In any case, there is nothing to be found on the website of ministries or the RIVM that indicates that the aim is to achieve an imperceptible or almost imperceptible level of infections.
On 23 June, the OMT published an advice that hovers between Strategy 3 and 4, but an advice is not a policy. It is a hopeful development that the political space to continue at level 2 has become smaller. Incidentally, RIVM 's explanation of 'maximum control' is another. See this screenshot taken on June 26th 2020.
The fact that there is serious discussion in journalism and society about which strategy the Netherlands is currently pursuing is already a strong signal for Strategies 1, 2 and 3, because containment requires clarity and broad support.
The conclusion is that the policy used to point to Strategies 1, 2 or 3, but there is now an OMT advice that points to 4 - the question now is whether this will become official policy.
2. Rhetoric
When we analyze the language used by decision makers, the picture becomes more cloudy. Until early June, Prime Minister Rutte repeated the above mantra on ICU-based mitigation and protecting the vulnerable as often as he was asked to explain. So strategy 1 or maybe 2. But since then, statements have been made as "as low as possible" level of infections. Also Van Dissel has spoken recently about "containment", "minimal virus" and "we will not circulate the virus." That gives the fans of containment some hope.
But at the same time, Sjaak de Gouw, the director of the umbrella organization of GGDs (regional public health units), recently came up with “ we want to make the virus land softly because otherwise we have no resistance to infections from outside” (read: building up immunity). Van Dissel also came up with “eventually there will be herd immunity or a vaccine” (read: we will not suppress it for as long as necessary).
You should also consider a statement such as “we do not want to stop the virus at all ” by OMT member Ann Vossen as policy until proven otherwise. The accelerated relaxations that we see now, while the R is already at 1.05 (according to the Ministry of VWS itself) do not necessarily prove an attempt to build up a little more immunity, but do prove that going to zero is not a priority.
The OMT advice of 23 June also points for the first time to 'containment' in the sense of reducing the number of infections to (almost) zero '
Conclusion: rhetoric has shifted from Strategy 1 and 2 to 3, with an opening visible towards Strategy 4
3. The signal values
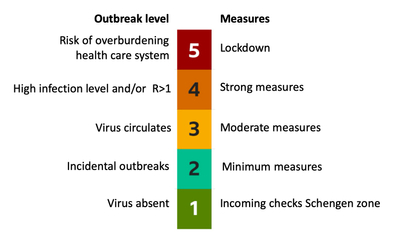
The government publishes a daily updated dashboard with signal values. This Dashboard leaves little to the imagination. Reproductiegetal = reproduction number, waarde = value, opnames = admissions and ziekenhuis = hospital.
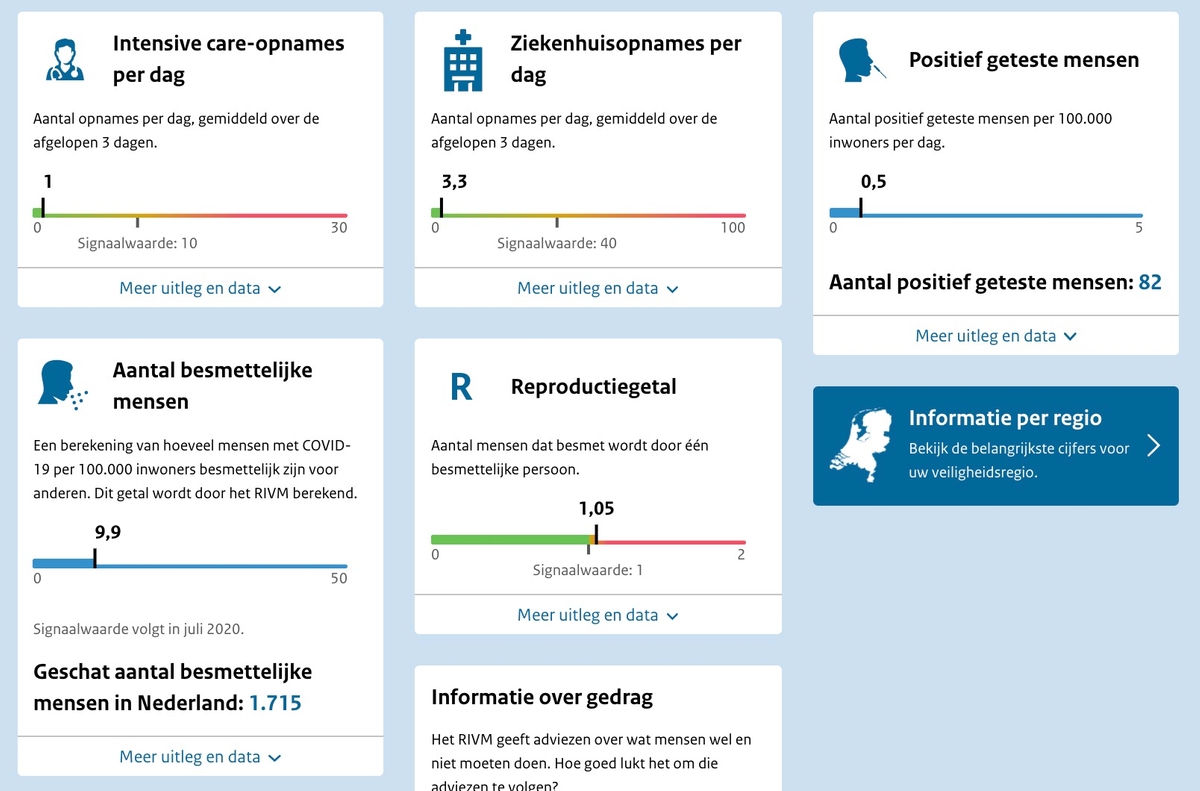
The reproduction number only turns orange just over 1 and everything below 1 is green. Countries that want Strategy 3 or 4 keep the R at 0.5 or 0.6 (and certainly not above 0.8) to quickly realize fewer infections and to minimize the risk of new peaks due to (very common) measurement errors .
The fact that 10 ICUs addmissions per day are not a problem is also only compatible with Strategy 2. Such a number (at 0.35% ICU) amounts to thousands of infections per day, a level that is so high that the rest of Europe would close its borders to the Dutch (unless, of course, inadequate testing hides the truth).
Conclusion: unmistakably Strategy 2.
4. Actions
If we analyze the actions of the government, it is striking that it is still policy to increase the number of ICU beds considerably . The healthcare sector is also negotiating new triage protocols for when hospitals become (almost) full again, as was the case in April. Both facts point to a policy aimed at a serious number of infections, because in suppression countries like New Zealand or Norway they are not afraid of large numbers of new Covid patients. Epidemiologically, the step from 200 people in ICUs to 2,000 is much smaller (and therefore more likely) than from 2 to 2,000.
The relaxation of the policy also leads to the belief that the government is gunning more at opening the economy than for maximum suppression of the virus. Open cinemas are virtually risk-free if you have a complete picture of where the virus is located; The Netherlands does not have this because we do not test enough and our contact research is not up to standard.
The cabinet has ordered a million antibody tests, which are especially useful for establishing immunity. The Cabinet's efforts to reserve priority vaccines for its own population also point to Strategies 1, 2 or 3, because if you suppress the virus you do not necessarily need a vaccine and probably not everyone will be choose cumbersome quarterly (?) vaccine shots, which makes such an intervention lose most of its purpose.
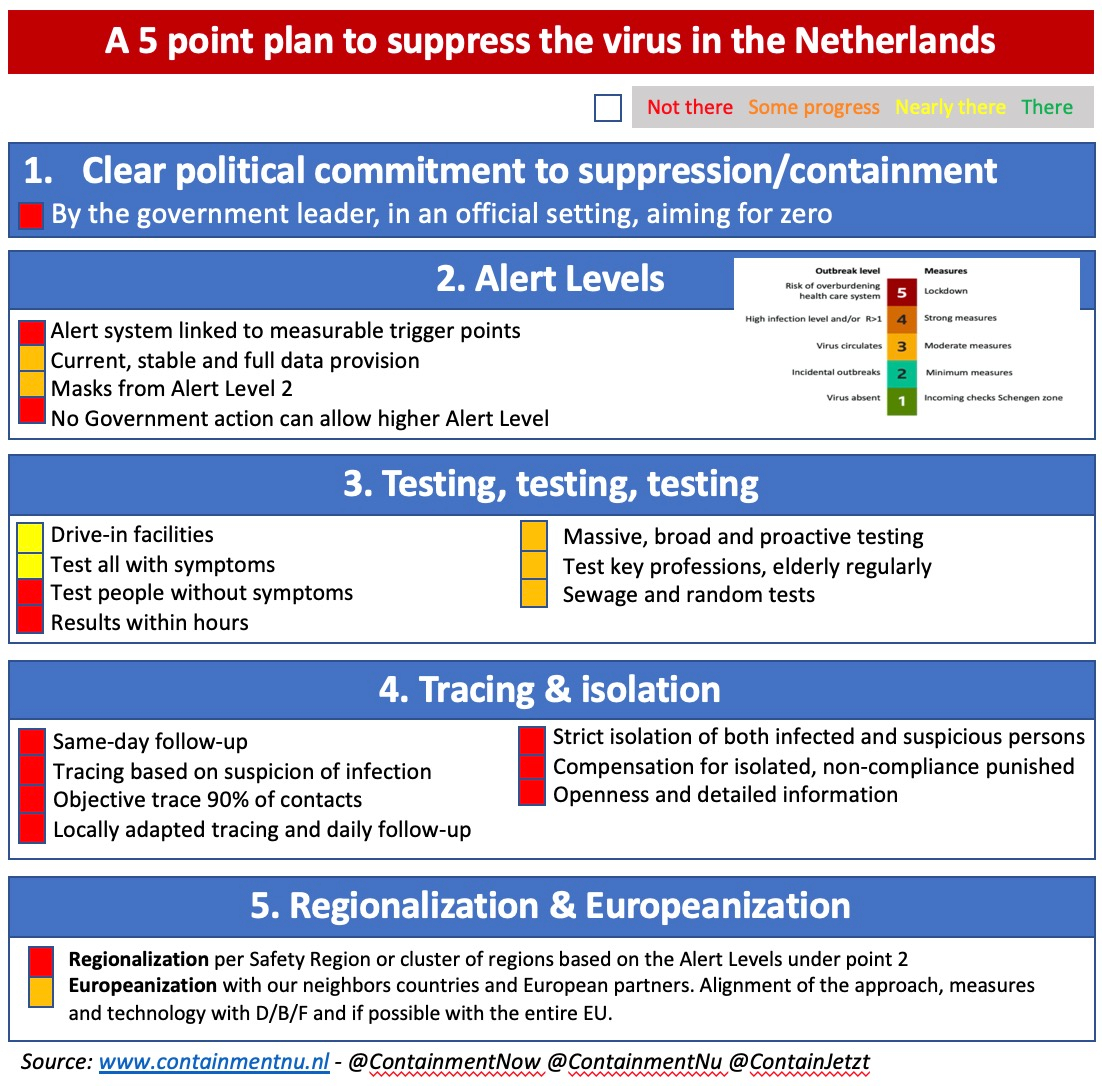
The scaling up of testing and the source and contact research (TTI) that has been underway since May has improved in quality, but is far behind that of other countries that are serious about getting rid of the virus. A quick look at our suppression dashboard that we maintain also shows the reddish colors of the spectrum. Not a dashboard that you would see in countries that really want to get rid of the virus.
There is steady improvement, according to the latest letter from the RIVM to the GGDs . TTI ambitions are being raised. The sewage water in all sewage treatment plants will also be checked soon (according to the government), which is an important method to prevent infection sources.
The conclusion is that government actions are not compatible with Strategies 4 or 1.
5. Communication and information provision
We have already said a lot about the misleading communication surrounding this policy. Whether it concerns the key points of tests, protective equipment or infectiousness of children, we have been misled and regularly lied to. That fits with a mitigation (virus spread) policy, because all those deaths are hard to sell to the public and people just expect the government to protect their bodies rather than claim them for some sort of medical experiment.
When Prime Minister Rutte said on June 4 that he had never made a speech about herd immunity, he told an astronomical lie, but one that fits with a slow change of course from Strategy 1 to 2 or 3 and possibly 4. The promise on 11 May by Public Health Minister De Jonge that “anyone who wants to can be tested from 1 June” has not materialized (very little was tested that day, the telephone lines were overcrowded and the test process still takes days to a week) but this seems to have more to do with incompetence than with false information.
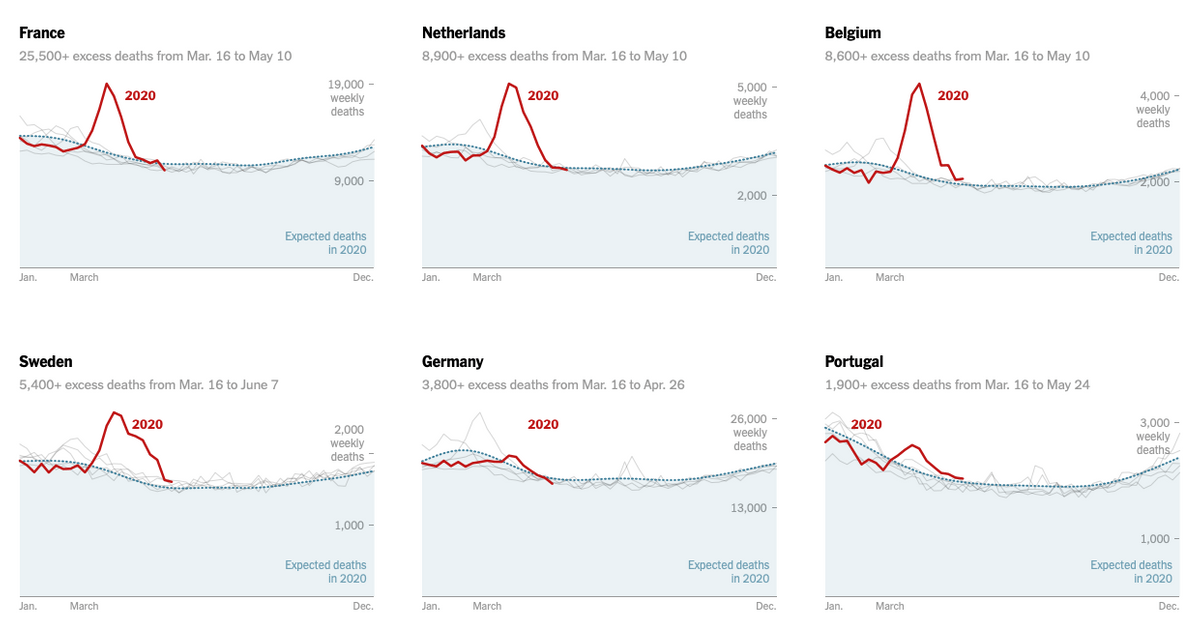
Over time the misleading has gotten less promiment, but the provision of information is faltering to such an extent that it is most congruous with an ongoing dissemination policy that seeks to conceal the damage it causes. The reports of positive tests per municipality have already been changed several times. The tally of ICU admissions from the RIVM is lower than the counts of the NICE Foundation , which also takes suspected Covid patients into account. RIVM has had a limited definition of what a Covid patient is since March and further tightened it up in May. This undercounts the number of deaths, even by a factor of 2, based on research by the New York Times, the Economist and the FT.
Such juggling of data is not common in countries that are seriously containing the outbreak, as trust and transparency are a high priority there. The Netherlands does not seem to take the virus as seriously (Strategy 3) or deliberately conceal the many negative consequences of the spread policy (Strategies 1 or 2).
The conclusion is that until the end of May the communication was congruent with Strategy 1 and 2, and since then with 2 or perhaps a poorly executed 3.
6. Results
The surest way to interpret policy is to measure it by results. If someone goes into the woods with a gun to "go for a walk" and comes out with two rabbits, he has probably been hunting. A mitigation policy (Strategies 1, 2 and 3) can be recognized by resulting in more infections (and therefore also sick and dead) than countries that seriously contain the outbreak.
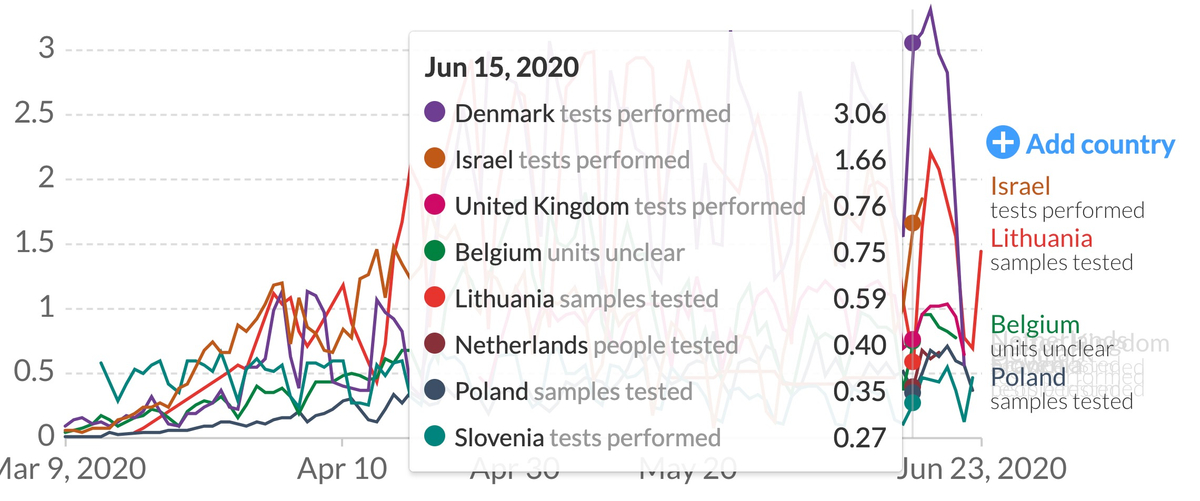
Unfortunately, the comparison is difficult to make because the Netherlands tests relatively little, and very litlle among children. In terms of mortality, the Netherlands is an outlier, with the late and relatively flexible measures introduced in March to curb the outbreak. But in June, that has not been so visible. However, this international comparison is also made more difficult by the change in definition of “Covid dead”, which is broader in other countries. In any case, the Netherlands currently has far more infections and hospital admissions than countries such as Slovenia and Luxembourg, which really would love to go to zero and stay there.
The definition of "excess mortality" (the number of people dying in a week in total in a week which is above normal will probably be Covid) was modified by CBS in May, which our analysts say has 1,500 to 2,000 people of excess mortality. "saved ”. So it is not easy to say that the Netherlands has many more deaths than other countries, but the flexible measures and open schools, just like the juggling with definitions and measurements, suggest that we clearly have more infections and deaths and therefore tolerate them.

The test results indicate that younger people are now becoming infected more often, which is appropriate for opening schools and opening places where young people gather. The isolation of older people is also working better and better, and indeed one of the few strict rules that remains is that grandchildren should not come close to their grandmother and grandfather, and that care homes can be visited sparingly. All of this is compatible with allowing significant infection in young people, who almost never reach ICUs, while the elderly stay stay as isolated as possible.
Conclusion: The results indicate a shift from Strategy 1 to Strategy 2.
7. Internal logic and interests
RIVM director Jaap van Dissel aimed for Strategy 1 in March, based on the observations of the outbreak in Wuhan: the fast sprint to some good herd immunity. Because that policy in itself leads to many deaths and has also been poorly implemented (underestimation of the virus and its dangers, no protection of the nursing homes, not taking into account the actual ICU capacity in the calculations) it is not easy change course. And because the policy was so "extreme" in March, this is an indication that RIVM will want to stay close to it in any case.
Conclusion: Strategies 2 and 3, maybe Strategy 1.
8. Reverse logic
If we turn around the question of which policy we are following, we quickly come to the conclusion that Strategy 4 is not on the table. The measures we have mentioned in our 5 point plan are popular in suppression countries (and among non-Dutch scholars and doctors), but almost completely absent in the Netherlands. The fact that the schools have opened almost fully (the fastest in Europe, as far as we know) without keeping a close eye on where the infections are (whilst that was promised) is a clear signal of building up immunity via the "cheapest" population group.
The Duch Cabinet will scale up TTI, but if they were really in a hurry, this could be top quality in a few weeks, for example by having external parties supplement the work of the GGDs. Testing can also be done in laboratories so that the GGDs have more time for contact research, but apparently other considerations play a role. The ICU capacity would not be scaled up in Strategy 4, no excessive effort would be made for a vaccine and seropositivity tests and Schiphol would carry out tests on incoming passengers. And Prime Minister Rutte would also have simply said that he wants to go to zero, instead of easing measures more quickly, as he is doing now.
Imagine that the government actually wants Strategy 1, but has no political space for it now. That too cannot be reconciled with what we see. TTI is indeed being improved. There has been talk of "as little virus as possible". And the Cabinet does indeed realize that a second major lockdown must be economically unthinkable.
Please note that the Netherlands may currently have many infections under the radar with its open schools, bars and many outdoor parties. Children under 12 are hardly tested and schools are not monitored structurally. If children are infected by the thousands at a time, you will not notice this in hospitals. Their parents will follow, but with a delay. And if you keep the elderly and vulnerable groups separate (at home), you can get a substantial immunity build-up without serious burden on the hospitals. This is in line with the policy of controlled dissemination, in which the children must first "be put on the slingshot", and then their parents and their friends.
Conclusion: Strategy 2 or 3.
General conclusion
If we try to reach the most "frugal" conclusion that does justice to everything that has been analyzed above, the policy floats between Strategies 2 and 3, with a development towards 3 and a first opening towards 4. The fact that the extremely destructive Strategy 2 and the totally destructive Strategy 1 are still “in play” or even conceivable is a major condemnation of government policy, both on moral grounds and because of the consequences for society and the economy.
If we analyze the actors, it seems that Van Dissel and De Gouw of the GGDs are still sitting on Strategy 2 and may very well hope for 1, although that would be extremely illogical. For them, TTI and mass testing are something unknown and something you do at the beginning, you still have to go for herd immunity and you want immunity to be able to open up the economy.
"There is now an OMT advice that strongly hints at Strategy 4, but the actions, communication and plans of the government are still in contradiction with this."
Rutte will have gone along with this in March, but we know from several very reliable insider (but non-Cabinet) sources that Rutte thought at the time that he would save the economy by allowing the virus to spread, but that he understands now that a second lockdown is the biggest risk. Rutte will therefore be able to live with very few infections (Strategy 3). Perhaps he even dreams of Strategy 4, but lacks the people with the backbone and resources around him to make that a concrete policy option.
And so the Netherlands is caught in the “Twilight Zone” between Strategies 2 and 3. There is now an OMT advice that strongly hints at Strategy 4, but the actions, communication and plans of the government are still in contradiction with this. That is not good enough for our country, because real suppression (Strategy 4) is by far preferable and urgent with autumn approaching. And we deserve that strategy for our well-being, for the economy and for our "vulnerable".
Analysis of the conclusion and the way forward
In a sense, ambiguity about the policy is also worse than simply betting on Strategy 3 (if Strategy 4 is not in the cards). By not fully using words and doing deeds compatible with Strategy 3 (or rather 4 of course) you will not get the GGDs and other government services moving at the fastest rate possible. The lack of clarity for the population also leads to a lowest common denominator effect: the people who think that everything is OK (“the virus is gone”, this is big now in Holland) do not follow the rules, and then the incentive for the rest to be strict disappears.
For example, the measures and our personal behavior (washing hands, keeping a distance, staying at home with complaints) are eroding. And now that the lack of clarity at least partly arises from internal tensions between RIVM and the government, and possibly also (parts of) the OMT, this makes careful and sharp analysis more difficult for our policymakers. Certainly also because there seems to be an informal or formal taboo in the media to expose the foundations of the strategy.
"The lack of clarity for the population also leads to a lowest common denominator effect"
And with that, the policy blur also reduces the pressure to move to Strategy 4. First of all, opposition is impossible. Newspapers do not want to publish criticism, because "we are already containing" or "containment is the same as controlled spread". People who might be able to be convinced by activists don't have the mental resources to think critically about the Strategies, which aren't even presented as different.
In a country like Germany that started with 2, quickly switched to 3 and is now trying 4, there is a logic and “flow” in the cabinet policy that is lacking in the Netherlands, now that we know nothing else than that the cabinet wants a lot of “control” which never existed. Our fear is that there will be a second peak in the outbreak, with very scary risks for our way of life. A fear that would be unreasonable in countries that go for Strategy 4.
Every citizen can and must therefore demand from MPs, their local GGD and (to influence the GGD) the city council that at least the policy is made clear. And if there is clarity, the battle can start to really ban the virus with world-leading TTI and, where necessary, additional measures such as masks in public areas and a ban on full events.